Passive protection.
Every case. Every day.
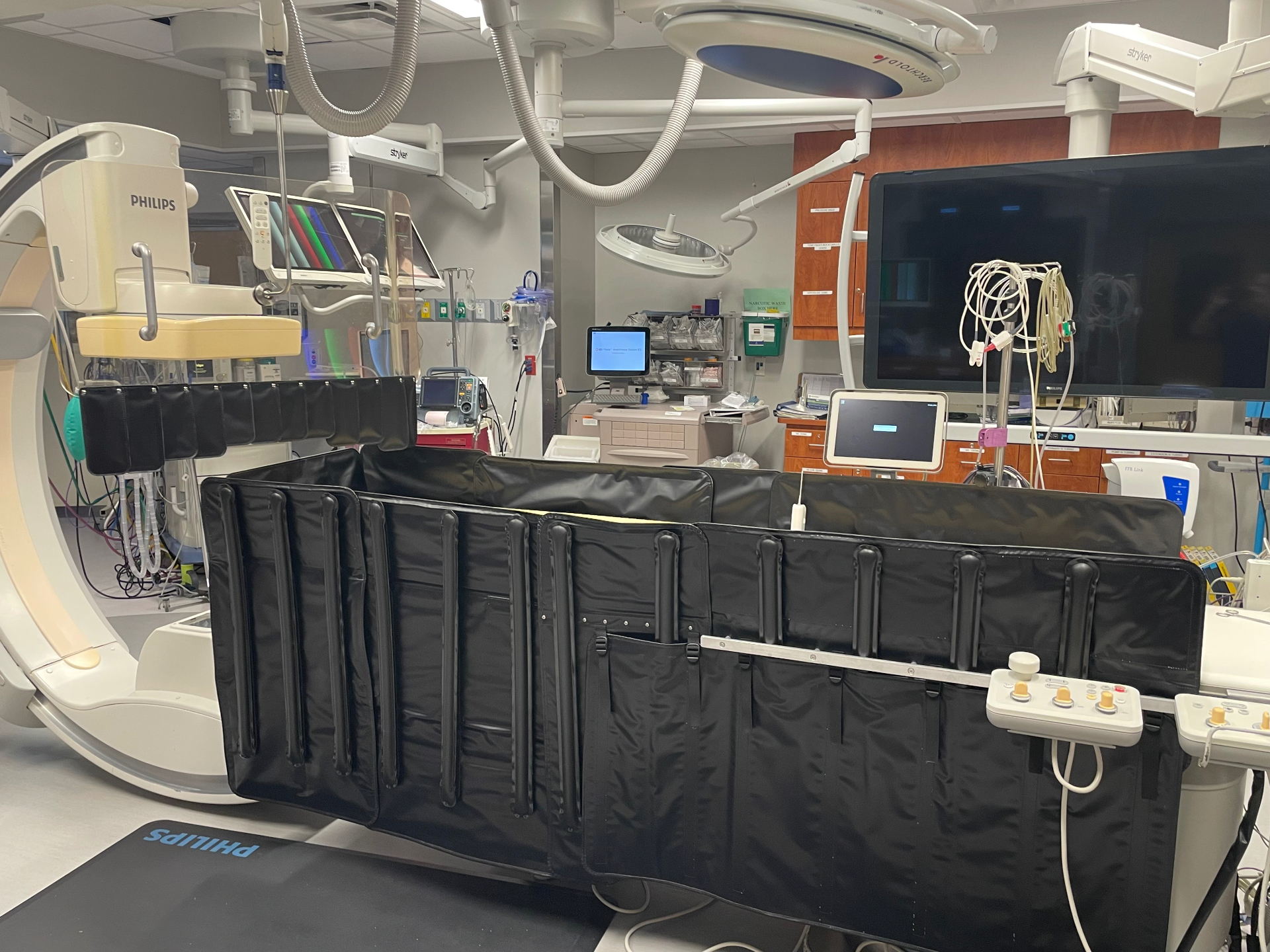
AeroShield™ pairs a table-mounted inflatable lower shield with the ceiling-mounted OptiShield™ to passively protect everyone in the lab — operator, scrub tech, anesthesia, and circulator — across the full range of imaging projections.
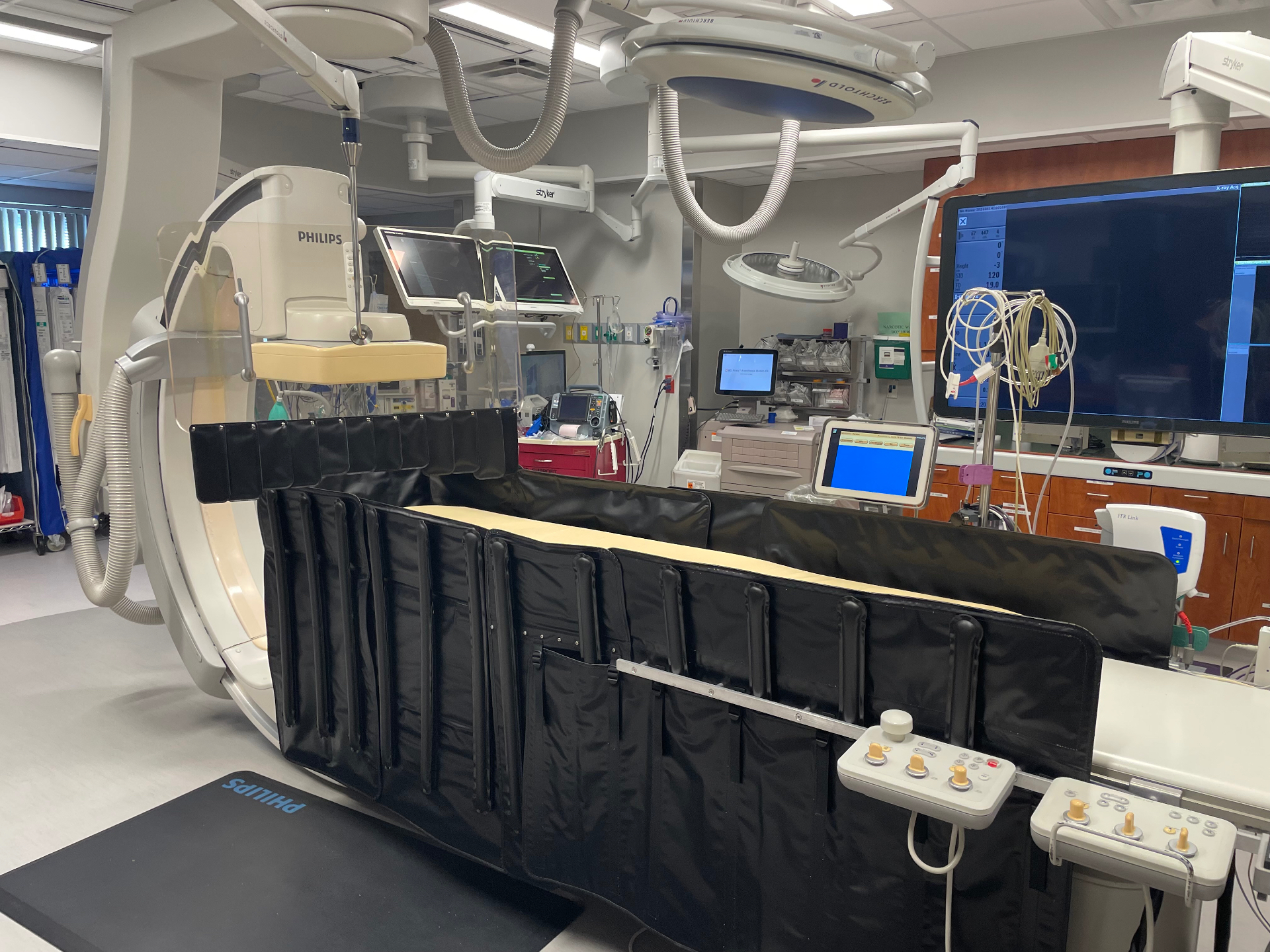
In the lab
See it deploy in under a minute.
Low-PSI air bladders inflate across all zones, the OptiShield™ drops into the boom arm you already use, and the team works exactly as they always have — with a continuous scatter barrier that doesn't depend on anyone's behavior.
The problem
Lead aprons protect one body part at a time.
Interventional cardiologists carry one of the highest occupational radiation doses in medicine — and so do the people standing next to them. Anesthesiologists, sedation nurses, and circulators are routinely left with little or no shielding at all.
Conventional setups depend on the operator remembering to reposition shields, hold a posture, or wear a heavier garment. AeroShield removes that dependency. Once the shield is in place, the protection is continuous.
The AeroShield™ system
A continuous barrier — not another piece of PPE.
Engineered with interventional cardiologists and radiation safety officers, AeroShield slots into the room you already have and protects the people doing the cases.
Innovative design
An inflatable lower shield plus the full-coverage OptiShield™ upper barrier reduce scatter across dynamic gantry angulations — including steep LAO.
Whole-team protection
Meaningful dose reduction for everyone in the room — primary operator, scrub tech, anesthesia, sedation nurse, and circulator.
Workflow integration
Passive protection after a quick inflation and OptiShield placement. Fast patient prep, easy cleaning, and clean room turnover.
Evidence
Clinically validated. Measured on real cases.
A prospective real-world comparison at Tallahassee Memorial Healthcare — 31 traditional cases vs. 30 AeroShield™ cases, every role measured with independent dosimetry. Validated against EDEX methodology per NRC Reg. Guide 8.40.
Clinical study — Tallahassee Memorial
61 cases · 5 staff roles · led by William Dixon, MD
PPE & policy
"Do we still have to wear lead?"
It's the first question every interventional team asks. The honest answer: that call belongs to your RSO and your state — and AeroShield™ is designed to make whatever they decide easier on your team.
Salus is building toward a future where the cath lab doesn't depend on a 15-pound apron to keep people safe. Until your program is ready to get there, we give you the tools to lighten the load now and the live data to know exactly where you stand.
Aligned with your RSO, not ahead of them
Lead requirements are set by your radiation safety officer, hospital policy, and state regulators — not by a vendor. AeroShield™ is built to deliver dramatic dose reduction inside whatever PPE protocol your program already runs.
If you still wear lead, wear less of it
Salus pairs AeroShield™ with GLiFT™ — a first-of-its-kind endoskeleton apron with rigid mantis bars that transfer the apron's weight from neck, shoulders, and spine onto the pelvic bone. Many wearers describe it as therapeutic. You keep your compliance posture; your spine gets a break.
Real-time dosimetry, in your hands
Every AeroShield™ deployment is paired with real-time dose monitoring across the team. We give your RSO live, role-by-role numbers — so the decision about what PPE your team needs is made on your data, not anyone's marketing claim.
The lighter lead option · GLiFT™
For teams not yet ready to step out of lead — wear less of it.
Endoskeleton, not just an apron
Proprietary rigid mantis bars transfer the apron's weight off the neck, shoulders, and spine — directly onto the pelvic bone. Adjustable belt with memory-foam padding and breathable spacer mesh.
- Unisex; includes thyroid shield, sleeves, reinforced front pocket
- Designed by clinicians, for clinicians
- 13 colorways · One F front-entry / One S side-entry
"It takes the weight off our spine and puts the weight on our hips."
"I was amazed at how much weight it took off the pain points in my body."
Product line



How it works
Fits the lab you already run.
- 01
Lower shield mounts to the rail
A low-profile, table-mounted inflatable shield sits flush against the procedure table — 38 lbs total system, fed by low-PSI (8 psi) air bladders with all-zone or per-zone control.
- 02
OptiShield™ drops into your existing boom
The above-table OptiShield (~25 lbs) attaches to the hanging shield boom arm you already have. No new rails. No ceiling work. Falls under the boom's weight load limit.
- 03
Inflate. Position. Work normally.
Once inflated and positioned, AeroShield protects passively across steep LAO, RAO, cranial and caudal angulations — including radial workflows with left and right kickouts.
- 04
Deflate in seconds for patient access
Soft material, no loss of patient communication. Deflates in seconds for emergency access, then re-inflates for the next case. No system to wheel away between patients.
"I didn't know it was there after a couple cases. I just worked as I normally would. When the Salus clinical team left after our study was complete, we've continued to use it in 100% of our cases. That's a testament to full adoption."
Built for
The people in the room.
Cath Lab Directors
Whole-team protection your program can stand behind — and a measurable lever against the long-term occupational liability of your operators.
Interventional Cardiologists
Cut your own scatter dose by ~95% per case. Two cases to full proficiency. Nothing in your hands changes.
Radiation Safety Officers
Independent bench study (NRC Reg. Guide 8.40, EDEX methodology) plus a prospective clinical comparison — drop-ready evidence for your annual ALARA review.
Request a consultation
Let's get your team fitted.
15 minutes with your Authorized Distributor for Salus Scientific. We'll walk you through the bench and clinical data and how AeroShield fits your existing room and boom arm.